The AE Adult Echocardiography Examination, administered by ARDMS, validates the clinical knowledge and technical competency required of a Registered Diagnostic Cardiac Sonographer. This exam assesses your ability to perform, interpret, and optimize adult echocardiographic studies in real-world clinical settings. Whether you are pursuing initial certification or renewal, this page provides a clear roadmap of exam content, question types, and effective preparation strategies. Understanding the syllabus and practicing with realistic scenarios will build confidence and improve your performance on test day.
Use this topic map to guide your study for ARDMS AE-Adult-Echocardiography (AE Adult Echocardiography Examination) within the Registered Diagnostic Cardiac Sonographer path.
The AE Adult Echocardiography Examination uses multiple-choice and scenario-based items to evaluate both foundational knowledge and clinical decision-making. Questions progress in difficulty and emphasize practical application to patient care.
Items are designed to reflect the complexity and decision points encountered during routine clinical practice, ensuring that your preparation translates directly to competent patient care.
Effective preparation requires a structured study plan that covers all five content domains and includes regular practice with realistic questions. Allocate study time proportionally to topic weight and your personal knowledge gaps, then reinforce learning through active recall and explanation.
Explore other ARDMS certifications: view all ARDMS exams.
Strengthen your preparation with up-to-date resources from validexamdumps.com. These materials align to AE-Adult-Echocardiography and cover practical scenarios with clear explanations.
Visit the exam page to download the PDF, Online Practice Test, or get Bundle Discount offer for both formats: AE Adult Echocardiography Examination.
Measurement Techniques, Maneuvers, and Sonographic Views and Pathology typically carry substantial weight because they directly reflect clinical practice. Anatomy and Physiology provides the foundation for all other domains, while Clinical Care and Safety and Instrumentation, Optimization, and Contrast are also tested but may represent a smaller percentage of items. Review the official ARDMS exam blueprint to confirm current topic distribution.
In practice, these domains work together seamlessly. You apply Anatomy and Physiology to recognize normal structures, use Instrumentation settings to optimize image quality, acquire views using proper Measurement Techniques and Maneuvers, interpret findings through the lens of Pathology, and maintain Clinical Care and Safety standards throughout. Understanding these connections helps you answer scenario-based questions that simulate actual patient encounters.
Most candidates benefit from at least one to two years of supervised echocardiography practice before attempting the exam. This experience builds pattern recognition and reinforces measurement accuracy. However, structured study of the five content domains and practice with realistic questions can help compensate for limited experience. Focus on understanding the "why" behind each measurement and interpretation, not just memorizing values.
Frequent errors include misidentifying acoustic windows or views, applying incorrect measurement guidelines, overlooking safety contraindications, and failing to optimize equipment settings before measuring. Many candidates also rush through scenario-based items without carefully reading all clinical details. Slow down, double-check your view identification, and consider the full clinical picture before selecting your answer.
Review your practice test results to identify persistent weak areas, then focus on those topics rather than trying to re-study everything. Take one final timed practice test to assess readiness and build confidence. Avoid cramming new material; instead, reinforce high-yield concepts and ensure you understand the rationale behind correct answers. Get adequate sleep, eat well, and manage test anxiety through relaxation techniques.
Which congenital abnormality is most consistent with the findings in this video?
The video shows an apical four-chamber or subcostal echocardiographic view demonstrating a markedly enlarged right atrium with atrialization of part of the right ventricle, displacement of the tricuspid valve septal leaflet downward into the RV cavity, and severe tricuspid regurgitation. These findings are hallmark features of Ebstein anomaly, a congenital malformation of the tricuspid valve causing apical displacement of the septal and posterior leaflets.
Patent foramen ovale and ventricular septal defects have different echocardiographic features without tricuspid leaflet displacement. Eisenmenger syndrome refers to advanced pulmonary hypertension due to shunts but is not a specific congenital structural abnormality.
These diagnostic criteria and echocardiographic hallmarks are described in adult congenital heart disease literature and echocardiography textbooks16:Textbook of Clinical Echocardiography, 6ep.570-57512:ASE Adult Congenital Guidelinesp.400-405.
Which of the following does this Image represent?
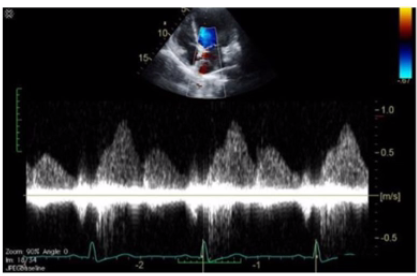
Comprehensive and Detailed Explanation From Exact Extract:
The image shows a pulsed-wave Doppler waveform with respiratory phasicity and distinct forward and reversed flow components characteristic of hepatic vein flow patterns. Hepatic vein Doppler typically displays a biphasic waveform with systolic (S) and diastolic (D) forward flow toward the heart and brief reversed flow during atrial contraction (A wave reversal), reflecting right atrial pressure changes.
Mitral and tricuspid inflow Doppler patterns show distinct E and A waves representing early and late diastolic ventricular filling but do not have the same flow reversal pattern. Pulmonary vein Doppler waveforms also differ, showing systolic and diastolic forward flows into the left atrium without the prominent reversed flow seen here.
The hepatic vein Doppler is commonly used in echocardiography to assess right atrial pressure and compliance, especially in conditions like constrictive pericarditis and right heart failure, where characteristic flow reversals and expiratory changes are observed.
This pattern and its clinical significance are detailed in adult echocardiography references, including the 'Textbook of Clinical Echocardiography' and ASE guidelines on Doppler imaging16:Hepatic Vein DopplerTextbook of Clinical Echocardiography, 6e12:ASE Doppler Guidelinesp.95-100.
A. Sinus venosus atrial septal defect
The echocardiographic image shows a typical atrial septal defect located in the central portion of the atrial septum, best classified as a secundum atrial septal defect (ASD). Secundum ASDs are the most common type, occurring in the fossa ovalis region.
Sinus venosus ASDs are located near the superior vena cava or inferior vena cava junctions, coronary sinus ASDs involve unroofing of the coronary sinus, and primum ASDs occur low in the atrial septum near the atrioventricular valves.
These anatomic distinctions are critical for diagnosis and surgical planning and are detailed in adult congenital heart disease and echocardiography references16:Textbook of Clinical Echocardiography, 6ep.565-57012:ASE Adult Congenital Guidelinesp.400-410.
Which of the following is commonly evaluated by the sniff maneuver?
Comprehensive and Detailed Explanation From Exact Extract:
The sniff maneuver is commonly used in echocardiography to assess right atrial pressure (RAP) indirectly by observing changes in the size and collapsibility of the inferior vena cava (IVC). During a sniff or rapid inspiration, negative intrathoracic pressure normally causes the IVC to collapse. The degree of IVC collapse during the sniff test correlates with RAP.
If the IVC is dilated and fails to collapse significantly with a sniff, this suggests elevated right atrial pressure, which can be caused by right heart failure, pulmonary hypertension, or volume overload.
This maneuver is not used to evaluate left atrial pressure or outflow tract obstructions, which require other echocardiographic parameters.
This assessment method is described in the 'Textbook of Clinical Echocardiography, 6e', Chapter on Right Heart Evaluation and Hemodynamics20:300-305Textbook of Clinical Echocardiography.
Which condition is most likely demonstrated by this M-mode image?
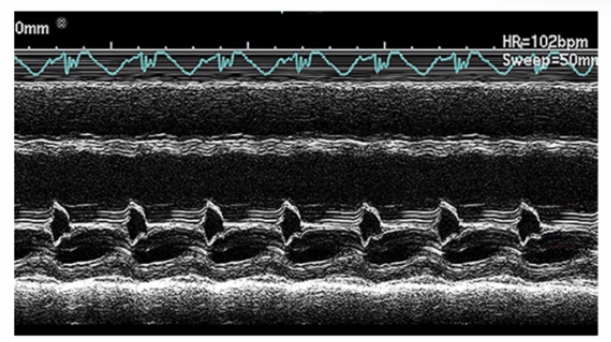
The M-mode image shows characteristic diastolic doming or ''hockey stick'' appearance of the anterior mitral leaflet with restricted leaflet motion. This is a classic sign of mitral stenosis, where leaflet thickening and fusion cause limited opening during diastole.
Dilated cardiomyopathy shows increased chamber sizes and decreased systolic function but not mitral leaflet doming. Hypertrophic cardiomyopathy is characterized by septal thickening and SAM of the mitral valve. Mitral valve prolapse shows leaflet billowing into the left atrium during systole.
This pattern is well described in ASE valvular heart disease guidelines and echocardiography texts12:ASE Valve Imaging Guidelinesp.180-18516:Textbook of Clinical Echocardiography, 6ep.200-205.