The AB-Abdomen (Abdomen Sonography Examination) is a core credential for sonographers pursuing ARDMS Registered Diagnostic Medical Sonographer certification. This exam validates your ability to perform, interpret, and report abdominal ultrasound studies with clinical accuracy and safety. Whether you're preparing for your first attempt or refining your knowledge, this page provides a clear roadmap of exam content, study strategies, and resources to build confidence. Use this guide to align your preparation with the official syllabus and focus on high-yield topics that directly impact patient care.
Use this topic map to guide your study for ARDMS AB-Abdomen (Abdomen Sonography Examination) within the Registered Diagnostic Medical Sonographer path.
The AB-Abdomen exam uses multiple question types to assess both foundational knowledge and clinical reasoning. Items progress in difficulty and reflect real-world scanning and interpretation challenges.
Questions are designed to reward both knowledge depth and practical judgment, ensuring that successful candidates can perform competently in clinical sonography roles.
An effective study plan distributes learning across the four core domains over 8-12 weeks, with progressive practice and self-assessment. Organize your time by topic, practice consistently with realistic questions, and refine weak areas before test day.
Explore other ARDMS certifications: view all ARDMS exams.
Strengthen your preparation with up-to-date resources from validexamdumps.com. These materials align to AB-Abdomen and cover practical scenarios with clear explanations.
Visit the exam page to download the PDF, Online Practice Test, or get a bundle discount for both formats: Abdomen Sonography Examination.
Anatomy, Perfusion, and Function and Pathology, Vascular Abnormalities, Trauma, and Postoperative Anatomy typically represent the largest portion of the exam. However, all four domains are tested, and mastery of Abdominal Physics and Clinical Care, Practice, and Quality Assurance is essential for safe, competent practice. Allocate study time proportionally but ensure no domain is neglected.
In clinical practice, you apply anatomy and physics knowledge simultaneously to optimize images, recognize pathology, and make protocol decisions. For example, understanding vascular anatomy guides your Doppler technique (physics), which helps you detect abnormal flow patterns (pathology) and document findings accurately (quality assurance). Study these domains as interconnected rather than isolated topics.
Clinical experience is invaluable for translating exam knowledge into competent scanning. Prioritize liver, kidney, pancreas, and aorta scans, as these organs appear frequently on the exam and are foundational to abdominal sonography. If your facility allows, seek additional scans of the spleen, bladder, and vascular structures to build comprehensive confidence.
Many candidates confuse similar pathologies, misapply physics principles to specific tissues, or overlook quality assurance and safety protocols. Others rush through scenario-based questions without fully analyzing the clinical context. Slow down, read each question completely, and consider how anatomy, physics, and pathology interact in each case.
In your final week, focus on review rather than new content. Retake practice tests, review questions you missed, and drill weak topic areas in short sessions. Avoid cramming; instead, maintain consistent daily study, get adequate sleep, and practice stress-management techniques. On exam day, trust your preparation and approach each question methodically.
Which vessel is located directly proximal to the origination of the renal arteries?
The renal arteries originate from the abdominal aorta just inferior to the superior mesenteric artery (SMA). The SMA arises anteriorly from the abdominal aorta at the level of L1, and just below it, the renal arteries branch laterally. The splenic vein, portal vein, and hepatic artery are located more superiorly in relation to the renal arteries.
According to Moore's Clinically Oriented Anatomy:
'The superior mesenteric artery arises from the anterior surface of the abdominal aorta just above the renal arteries.' (Moore KL et al., Clinically Oriented Anatomy, 8th ed.)
Moore KL, Dalley AF, Agur AMR. Clinically Oriented Anatomy. 8th ed. Wolters Kluwer, 2018.
Gray's Anatomy for Students, 4th ed., Elsevier, 2019.
Which condition is most likely the cause of claudication experienced two weeks after this image was obtained?
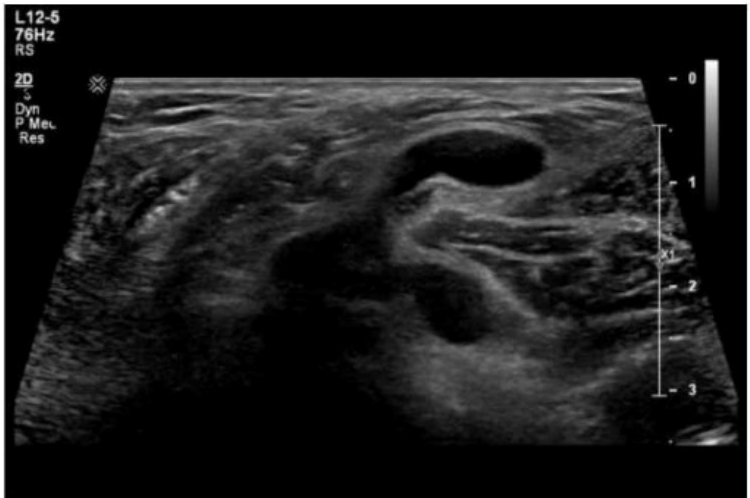
The ultrasound image demonstrates a fluid-filled structure in the posterior knee region, consistent with a Baker cyst (also called a popliteal cyst). A Baker cyst is a synovial fluid-filled sac arising from the posterior medial aspect of the knee joint, typically extending between the medial head of the gastrocnemius and the semimembranosus tendon.
The history of delayed-onset claudication (pain in the calf when walking) two weeks after this image was obtained is strongly suggestive of a ruptured Baker cyst. When a Baker cyst ruptures, synovial fluid may track inferiorly into the calf, producing pain, swelling, and clinical symptoms that mimic deep vein thrombosis (DVT) or arterial insufficiency (e.g., pseudothrombophlebitis syndrome).
Ultrasound findings consistent with a ruptured Baker cyst:
Complex fluid collection tracking along muscle fascial planes (hypoechoic to anechoic)
Posterior calf swelling and tenderness
Absence of thrombus in the deep venous system
Crescent-shaped fluid may be seen between muscle compartments
Why the other choices are incorrect:
A . Neuropathy: Would not show fluid-filled structures on ultrasound and would not present with calf swelling.
B . Infected hematoma: May appear complex, but would require a history of trauma or anticoagulation and systemic signs (fever, redness).
C . Thrombophlebitis: Involves a thrombosed superficial vein with wall thickening and surrounding inflammation, which is not seen in this image.
American Institute of Ultrasound in Medicine (AIUM). Practice Guidelines for Musculoskeletal Ultrasound Examination, 2020.
Bianchi S., Martinoli C. Ultrasound of the Musculoskeletal System. Springer, 2007. Chapter: Knee Region --- Popliteal Fossa and Baker's Cyst, pp. 433--437.
Radiopaedia.org. Ruptured Baker cyst: https://radiopaedia.org/articles/ruptured-bakers-cyst
Which finding is helpful to differentiate postsurgical breast scarring from a recurrent tumor?
Postsurgical breast scarring may appear hypoechoic and irregular but typically shows no internal vascularity on Doppler imaging. In contrast, recurrent tumors generally exhibit increased internal vascular flow due to neovascularization. Therefore, absent Doppler signal helps suggest scar tissue rather than malignancy.
According to Stavros' Breast Ultrasound:
''The absence of internal Doppler flow favors scar tissue, whereas recurrent malignancy typically demonstrates internal vascularity.''
Stavros AT. Breast Ultrasound. Lippincott Williams & Wilkins, 2004.
AIUM Practice Parameter for Breast Ultrasound, 2020.
---
Which finding is most likely demonstrated in this abdominal wall image of a patient with a history of atrial fibrillation?

The ultrasound image demonstrates a complex, heterogeneous hypoechoic collection within the abdominal wall, with mixed echogenicity and ill-defined margins. The lesion appears to contain internal debris but lacks definitive signs of vascularity or air (which would be seen in an abscess). There is no peristalsis, herniated bowel, or fat to suggest hernia.
Given the history of atrial fibrillation --- a condition commonly treated with anticoagulation therapy (e.g., warfarin, apixaban) --- this clinical background raises high suspicion for a rectus sheath or abdominal wall hematoma.
Key ultrasound features of hematomas:
Early (acute): hyperechoic or heterogeneous
Chronic/resolving: complex or cystic with fluid-debris levels
No internal vascularity on Doppler
May be confined to muscle or fascial planes
This is consistent with a hematoma, particularly in patients on anticoagulation therapy.
Comparison of answer choices:
Hernia --- typically shows bowel or fat with movement/peristalsis passing through a fascial defect.
Lipoma --- usually homogeneous and echogenic, not complex or fluid-filled.
Abscess --- often presents as a complex fluid collection with peripheral hyperemia and possibly air, plus systemic signs of infection.
Hematoma --- Correct. The image and clinical history (anticoagulation due to atrial fibrillation) strongly support this diagnosis.
Berman L, et al. Sonographic appearance and evolution of rectus sheath hematomas. AJR Am J Roentgenol. 1996.
Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic Ultrasound, 5th ed. Elsevier; 2017.
AIUM Practice Parameter for the Performance of Diagnostic Ultrasound Examinations of the Abdomen and Retroperitoneum (2020).
The absence of which sonographic finding indicates the acute process depicted in these images?
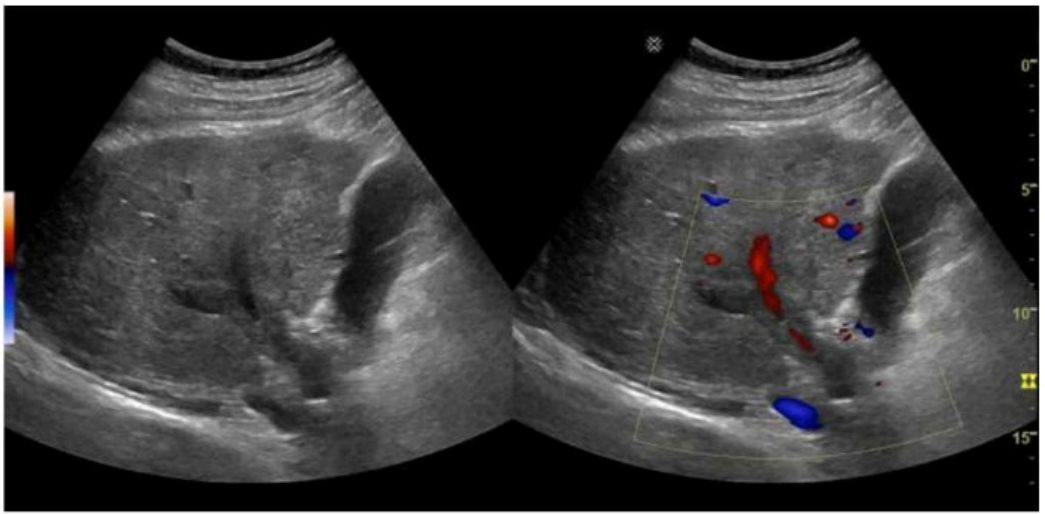
The sonographic images depict an acute thrombotic process involving the portal venous system. The absence of cavernous transformation in the setting of portal vein thrombus indicates that the process is acute. In chronic portal vein thrombosis, collateral vessels form in the porta hepatis to bypass the obstruction, a process known as cavernous transformation.
Sonographic features suggesting acute portal vein thrombosis:
Echogenic thrombus within the portal vein lumen
Absence of flow on color Doppler
Enlarged portal vein diameter early in the process
No evidence of cavernous transformation (i.e., no serpiginous collateral vessels at porta hepatis)
Cavernous transformation is a hallmark of chronic portal vein thrombosis and takes weeks to months to develop. Therefore, its absence on ultrasound supports an acute diagnosis.
Differentiation from other options:
A . Free fluid: Non-specific and may or may not be present in hepatic vascular thrombosis.
B . Ductal dilatation: Related to biliary obstruction, not portal or hepatic venous thrombosis.
C . Hepatic vein thrombosis: Seen in Budd-Chiari syndrome, which affects hepatic outflow, not portal inflow.
Rumack CM, Wilson SR, Charboneau JW, Levine D. Diagnostic Ultrasound. 5th Edition. Elsevier, 2018. Chapter: Portal Venous System, pp. 105--108.
American Institute of Ultrasound in Medicine (AIUM) Practice Parameter for the Performance of Hepatic Doppler Ultrasound Examinations, 2020.
Radiopaedia.org. Cavernous transformation of the portal vein: https://radiopaedia.org/articles/cavernous-transformation-of-the-portal-vein